FAQs
My eyes are often uncomfortable or sore. How can I tell if I have Dry Eye Syndrome?
There are many things that can cause an uncomfortable eye – usually some agent, either outside the eye or a side-effect of any medication being taken. To find out if you may have Dry Eye Syndrome, please fill out the following questionnaire and a clinically experienced optometrist will come back to you … but you must leave an email address for us to contact you. This may take up to 48 hours.
How can I make my dry eyes more comfortable?
There are a number of things you can do to ease your symptoms or prevent dry eye syndrome but its best to call in to see us to confirm that you have Dry Eyes and not another problem. For those people who experience watery eyes, especially when out in the cold, this is a common feature of Dry Eyes! The oily secretions produced by the eyelids are not producing enough oil to coat the tears and so the surface of the eye dries out a little. The tear glands react by producing more tears to compensate for the surface dryness … and because the eye’s natural drainage cannot cope with this extra volume, the tears overflow onto the cheeks. What can make this process worse is when lower lid margin becomes rippled due to dropout of the tiny holes through which the natural oils pass. Correct treatment and regular lid hygiene can prevent this happening – so make an appointment to see one of our specialists .
Environmental Facrors
Certain environments can irritate your eyes. Keep your eyes protected from.
- wind
- hot air
- smoke
Wrap-around glasses may provide good protection. Avoid smoky environments and if you smoke you should try to stop. Do not use eye make-up. This is easy to say but difficult advice to give! Eyeliner and mascara will block the special glands in the eyelids and can cause a toxic inflammatory reaction.
Specialized eyeware
Some cases of dry eye disease can be treated using specialised eyeware. These include specially made glasses called moisture chamber spectacles. These wrap around your eyes like goggles, helping to retain moisture and protecting your eyes from irritants. They are expensive but effective. EyeBags are more cost-effective and come in a starter pack following an initial assessment at our Dry Eye clinics. If your contact lenses were (or are) causing dry eye disease, special contact lenses are also available that may allow better oxygen flow into the eyes that your current lenses. You should discuss various options with our expert clinical optometrists.
Adjust your computer
Make sure that your computer workstation is positioned correctly to minimise eye strain. If you are using a computer at work, most employers have a health and safety officer or an occupational health representative who can advise you about this. Your monitor (screen) should stand at eye level or just below it. If you use a computer, make sure that you take enough breaks away from your computer screen and blink your eyes regularly. Taking breaks every hour to “rest” your eyes may help reduce your symptoms. Blink exercises are important since they not only help lubricate the eyes regularly, eliminating dry patches, but also help express lid margin oils that coat the eye.
Use a humidifier
A humidifier at work and home will moisten the surrounding air. Opening windows for a few minutes on cold days and longer in spring and summer will also help keep air moist and prevent build-up of mould.
Keep your eyes clean
Good hygiene will help improve dry eye syndrome, particularly if you have blepharitis (inflammation of the eyelids). There are three main steps to eyelid hygiene that should be performed once or twice a day.
- warm compresses
- gentle eyelid massage
- lid margin hygiene
Warm compresses
- Soaking a clean flannel or eye pad in the warm water and gently placing this over the eyes for around 10 minutes was the original advice.
- The warmth from the flannel is not enough to melt the oils in the stagnated meibomian glands of the eyelids.
- A microwavable “eyebag” is the recommended method, together with antibiotic lid wipes and eye lubricants.
Eyelid massage
- After you have used the carefully heated EyeBag on the eyelids for about ten minutes.
- Gently massage your closed eyes by rolling your little finger in a circular motion – this will help to push the melted oil out of the glands. You cannot see the oil come out, as the droplets are tiny.
- Next, take a cotton-tipped applicator (cotton wool bud). With your eyes shut, gently roll the cotton bud downwards on the upper eyelid towards the lashes and eyelid margins, then repeat along the whole length of the upper eyelid. This will help express the residual oil out of all the glands.
- Repeat expression for the lower eyelid glands by rolling a clean cotton-tipped applicator upwards towards the lashes and the eyelid margin.
- If the oils have been stagnant in the glands for quite some time, they might have changed their chemical structure. It is possible that when the oil drains onto the surface of the eye after gentle expression, it might cause irritation, a bit like getting soap in your eyes. This is normal and should get better with time as the blepharitis comes under control.
Lid margin hygiene
- The expressed oils should be wiped away from the eyelid margin. This also helps to reduce bacteria, dust or grime that might have accumulated along the eyelids while blinking, and also any remaining crusts.
- Do not use baby shampoo, as this is fragranced and can make things worse.
- Dip a clean cotton-tipped applicator into Blephagel and gently clean the eyelid margins by wiping the cotton bud along the rims behind the roots of the lashes, the bases of the lashes and the lengths of the lashes.
- Alternatively, BlephaClean sterile lid wipes can be used. These wipes are an excellent replacement for lid wipes that you may use at night to remove your makeup since they have the dual purpose of removing your makeup at the same time as removing any eyelid debris left over from Blepharitis or the day’s normal collection of debris.
If your problem is not caused by evaporative dry eyes, your doctor might prescribe an antibiotic ointment to rub along the eyelid margins after the three-step lid hygiene regime. This is usually used only for a short period of time. If there is inflammation, anti-inflammatory eye drops or tablets may be required.
Diet
There is increasing evidence that suggests a diet high in omega-3 fats can help improve ocular surface health, meibomian gland function and dry eye disease. This also has a wide range of health benefits, including reducing the risk of heart disease, joint problems and macular degeneration. The most important omega-3s are.
- eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) – both found in wild fish
- alpha-linolenic acid (ALA) – found in green leafy vegetables, flaxseed, soya beans, canola oil and walnuts
However, it is important to maintain a balance with omega-6 fatty acids, found primarily in vegetable oils, red meat-derived saturated fats, fast foods, evening primrose oil and borage oil. The best way to redress the omega-3 versus omega-6 balance is to increase oily fish intake, such as.
- mackerel
- salmon
- sardines
- herring
- fresh tuna (not canned, as the canning process removes the beneficial oils)
Aim to eat at least two portions of fish a week, one of which should be oily fish. Omega-3 supplements are also effective.
What is the treatment of Age-related Macular Degeneration?
Age related Macular Degeneration is a leading cause of blindness in the Western World. Treatment can be difficult and, in the wet form, may involve intravitreal injections or laser treatment.
Latest Treatments:Anti-VEGF Intravitreal injections
Avastin (Bebacizumab) and Lucentis (Ranibizumab) are new anti-vascular endothelial growth factor (VEGF) drugs, which have shown great promise in treating macular diseases such as macular degeneration and macular oedema. They have also been useful in cases of diabetic retinopathy and central retinal vein occlusion. These drugs act by inhibiting the growth of abnormal blood vessels and help prevent leakage of these blood vessels. In macular degeneration they are useful in the wet type of macular degeneration in which abnormal blood vessels grow in the retina at the back of the eye. These vessels cause leakage of blood or fluid that result in blurred or distorted vision. The aim of treatment with these anti-VEGF intravitreal injections is to stop the leakage and prevent further damage. Current research has found these drugs to be well tolerated as an intravitreal injection. Research so far has demonstrated that up to 70% of patients can show improvement with this treatment. Further research is showing good promise in cases of diabetic retinopathy and cases of persisting macular oedema, such as in central retinal vein occlusion. Injection of these drugs is performed as an outpatient procedure. Topical and local anaesthetic is used and therefore the injection should have minimal pain. Patients are discharged on the same day and may go home with a patch on their eye. This is removed after approximately three hours and antibiotic eye drops are administered four times a day for one week to help prevent infection. Patients need to be aware that in the first one or two days they may have some ocular irritation from the injection, as well as a tearing and redness of their eye. They should notify the Doctor or ophthalmologist if they notice persisting pain beyond 2 days or sign of infection or severe loss of vision. Generally the side affects of these drugs are rare but can include intraocular infection, which can cause loss of vision and requires urgent treatment. Also very rare complications include lens damage, retinal detachment and very rarely blood pressure rise, stroke, and cardiovascular problems.
Most patients require injection performed monthly for the first three months, often requiring OCT Scans to monitor the progression. Following this, the interval between treatments may be increased up to three months. Treatment will be tapered by your ophthalmologist according to the response that is obtained. Some patients have responded very well and only require one or two injections, whereas others have required repeated injections before they are stabilised. Average is approximately 6-7 treatments per year. Avastin is an expensive drug. it was originally developed for treatment of colon and rectal cancer but was found to have excellent benefit as an individual injection in the eye and therefore usage has continued with this. Several thousands of cases have been performed with no significant adverse outcomes. Lucentis, another drug of treatment derived from Avastin, has undergone extensive research and appears to have the same clinical effectiveness in the eye. The molecule of Avastin is larger than Lucentis and may have a longer action in the eye, though Lucentis does supposedly have increased effectiveness though reports have suggested little difference in their clinical affect.
Are eye vitamins of any use?
The use of antioxidant vitamins, such as Viteyes, Macugen and Ocuvite, has been reported to be useful in reducing the progression of macular degeneration by reducing oxidation damage to the retinal cells. Patients may take one or two of these eye-targeted vitamins ampules each day as instructed by their optometrist. There also is some new research into Omega 3 vitamins, which may also help to protect the eyes. A diet including fish, green vegetables and nuts is beneficial. Use of margarine, cooking oils (except olive oil) and processed food should be avoided. Smoking has also shown increased risk of macular degeneration progression and should be ceased. A ground-breaking, ten year study conducted by the US National Eye Institute proved that a high dose of specific vitamins and minerals (vitamins A (as beta-carotene), C, E, zinc and copper) could help reduce the risk of developing certain age related macular changes. The Royal College of Ophthalmologists Interim Recommendations for the Management of Patients with Age-related Macular Degeneration (AMD) – AMD Interim Guidelines – version 3: Nov2007 states that a product based on this formula should be recommended to patients at risk of development of Age-related Macular Degeneration. Other research conducted by the US North Chicago VA Medical Centre and other smaller scale studies has demonstrated that the carotenoid lutein has an important role to play in maintaining visual performance and macular health. Researchers at the Watford Clinic at the Institute of Vision Research in Ireland have pointed to a gene that increases the risk of its carrriers for AMD and cites the importance of Meso-zeaxanthin in the health eye-friendly diet.
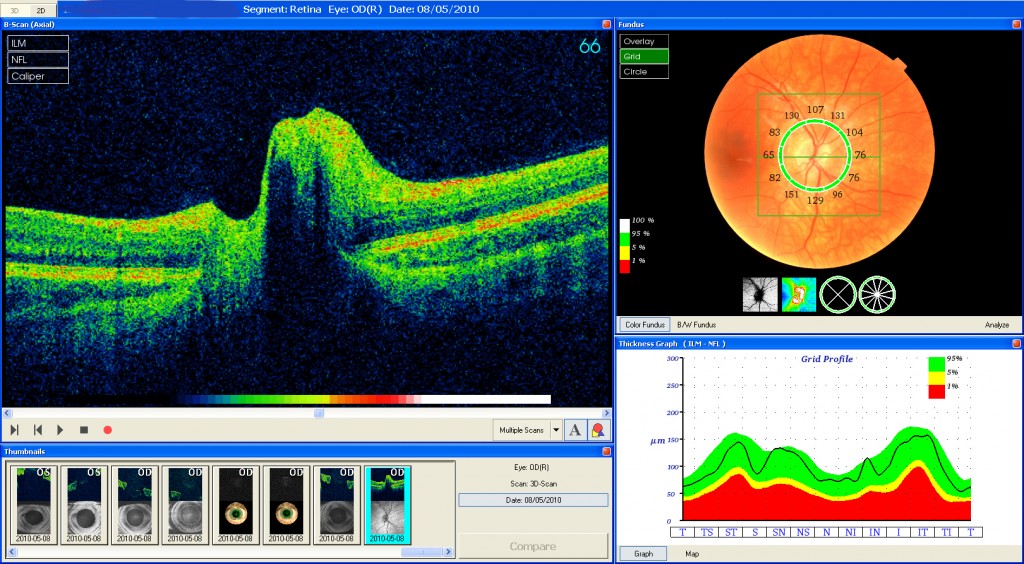
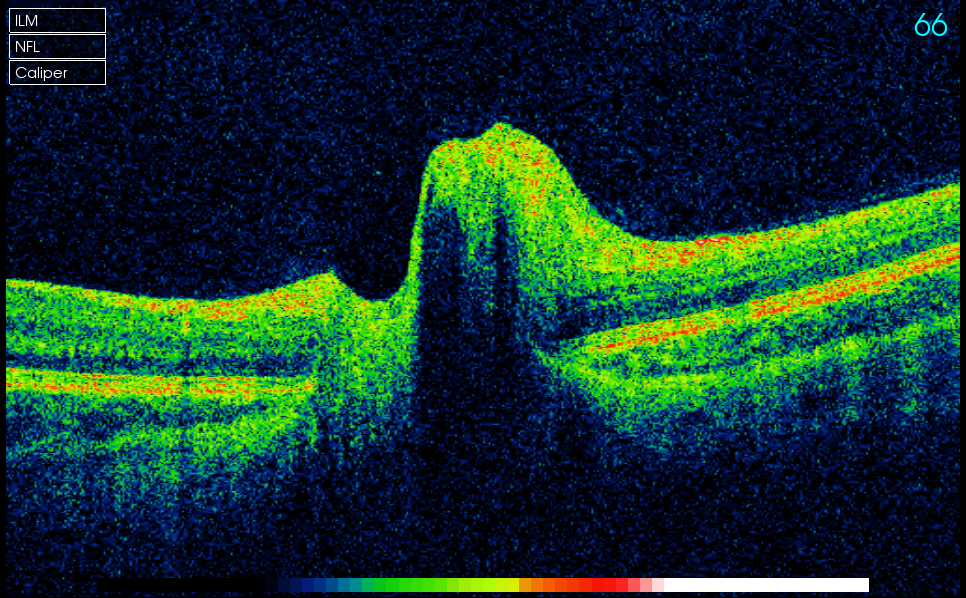
Besides macular degeneration, what will the OCT be able to detect?
Vitreomacular traction can clearly be diagnosed through OCT providing invaluable information as to the current relationship between the vitreous and the retinal surface. As we get older the vitreous, the jelly that takes up the space in our eyeball, can change. It becomes less firm and can move away from the back of the eye towards the centre, in some cases parts do not detach and cause ‘pulling’ of the retinal surface. The danger of a Vitreous detachment is that there is no pain and your eyesight will seem unchanged but the back of your eye may be being damaged. This pulling of the retina resembles cling film and is often termed ‘cellophane’ maculopathy and is clearly seen, even at a very early stage, by OCT imaging. Early retinal holes and macular swelling lend themselves well to being scanned since their pathophysiology is quite evident when the retina is ‘sliced’ sideways with the scanning beam.
Early glaucoma is characterised by changes in the thickness of bunches of nerve fibres that course down the tube that, collectively, we call the optic nerve. Not only can the OCT see this depletion in nerve fibre layer but has the capacity to measure the space between the accumulation of nerve fibres travelling down the optic nerve. Change in the volume occupied by this space, the optic cup, is often a first sign of nerve fibre damage – early glaucoma. The OCT can measure this volume change over a period of time and an increase in this cup volume is suggestive of nerve fibre layer death. This alerts the clinician to the possiblity of glaucoma earlier than may be detected by human observation alone. Tumors under the central retina can be imaged by the OCT and any ‘freckle’ that has been identified can be monitored for change in thickness and size more easily by a time-sequence of images.
I am 75 years old – can I wear contact lenses?
Yes – providing your eyes are not too dry. Age is NOT a barrier to wearing contact lenses… but confidence IS. We have plenty of experience in contact lens management to ensure that we give you confidence to wear your contact lenses.
Tell me more about contact lenses
Contact lenses are one of the miracles of modern technology. Today, more than three million people in the UK enjoy the clear, natural and unobstructed vision offered by contact lenses which don’t fog up or get splashed with rain as glasses sometimes can.
New lens designs and materials, as well as advanced care products, now make contact lenses easier and more comfortable to wear than ever before. They offer freedom from wearing glasses in daily life, when playing sport, or for that important social occasion, and can bring particular benefits for individuals with stronger vision correction requirements.
Are contact lenses right for me
Major advances in contact lens design mean that almost everyone can wear contact lenses successfully nowadays. People of all ages can be fitted, although special care is needed for the very young and elderly. Common eyesight defects, such as short-sightedness and long-sightedness, are easily corrected with contact lenses, but now conditions such as astigmatism and presbyopia (needing glasses for reading, too) can also be treated very effectively with contact lenses.
In the past, people with astigmatism, a condition in which the eye is irregularly shaped causing distorted vision, were restricted to wearing glasses, but today’s ‘toric’ contact lenses can be custom made for each individual to provide clear vision. Presbyopia, the ageing of the eye’s lens that progressively affects everyone over the age of about 40, makes it difficult to shift focus between near and distant objects. This condition can also be corrected with bifocal (or, more usually, multifocal) contact lenses that provide clear distance and near vision.
As contact lenses float on the tear fluid and do not actually touch the eye, there is no discomfort and nothing to obstruct your peripheral vision in the way that spectacle frames can. Also, the lenses move with your eye, meaning that you are always looking through the centre of the lens, where vision is best. In the majority of cases, people actually see better with contact lenses than they would with glasses.
What should I do if I want to try contact lenses?
Before you can wear contact lenses you must have your eyes fully examined. All our practices have contact lens practitioners who are qualified to fit and dispense contact lenses. During the examination your eyes will be tested to determine the strength of lenses you will need for clear vision, and the health of you and your eyes and eyelids will be examined. The quality of your tears, needed for lubrication of contact lenses – will also be assessed. Then, the curvature and diameter of the cornea at the front of your eye will be measured, together with the size of your pupils and the positions of your eyelids. Based on this information, your practitioner will be able to advise you about the most suitable contact lenses.
What type of contact lenses are available?
Hard lenses The first contact lenses were what have become known as ‘hard’ lenses. These are/were made of a perspex material that, while very durable, did not allow essential oxygen to pass through to the surface of the eye. Although still available for certain specialist needs, they have been largely replaced by gas permeable lenses that allow good oxygen flow and enable the eye to ‘breathe’.
Rigid gas permeable (RGP) lenses
Rigid gas permeable lenses allow oxygen to pass to the surface of the eye, but they are made of firmer plastics than soft lenses. This makes them more durable and gives them a longer life span. These lenses are particularly suitable for certain prescriptions such as high degrees of astigmatism, where they give very good vision. Some people find rigid lenses easier to handle than soft lenses and, although they take a little longer to get used to, regular wearers find them very comfortable.
Soft lenses
Modern soft contact lenses are made from gel-like plastics, often with a high water content, that allow oxygen to pass freely to the eye. Because of this, soft lenses can be made much larger which in turn makes them very comfortable and easy to adapt to. Some of the new ultra-thin soft lenses are so comfortable that new wearers can leave them in all day right from the start. New users usually find that they are only mildly aware of standard thickness soft lenses and that tolerance can be built up fairly easily so that most people are able to wear them all day within a week. Newer materials, such as Silicon Hydrogel (SiH), allow previously-unsuccessful wearers and those with ‘dry eyes’ to wear contact lenses.
Disposable lenses
All types of contact lenses are now available on a planned replacement programme. New manufacturing techniques have made it possible for users to have a fresh pair of lenses regularly for about the same cost over a period as non-disposable lenses. Daily disposable lenses are becoming increasingly popular as they eliminate the need for a lens care routine, but depending on the type of lens and the environment in which it will be worn, the replacement period can be anything from one day to two years.
Extended wear lenses
Most contact lenses are worn on a daily basis, being removed in the evening and put back in next morning. Special extended wear soft lenses are now available which may be recommended by your practitioner, which allow you to sleep in them. Typically they are replaced weekly or monthly.
Tinted lenses
Exciting tinted contact lenses that can enhance or even change the colour of your eyes without affecting what you see are now widely available.
Are contact lenses difficult to insert and remove?
No. Many people are worried about putting a lens in for the first time, but simple techniques have been developed which make insertion and removal of contact lenses quite easy. When you get your lenses you will be taught the correct method and will not be allowed to take them home until both you and the practitioner is confident that you will be able to safely insert and remove your lenses.
Caring for your lenses
Developments in lens care products have now made it easier than ever to keep your contact lenses clean, comfortable and safe from harmful bacteria. These three simple steps should result in trouble-free use:
- Clean your contact lenses daily
- This will remove dust, pollution, make-up and other things that may accumulate on the lens in daily wear.
- Disinfect your contact lenses daily
- Disinfecting your lenses will ensure they are free from any micro-organisms still on the lens after cleaning.
Weekly protein removal - This breaks down protein deposits that are produced naturally in everyone’s tears. If you don’t do this the performance and life of the lens could be reduced. Your practitioner will advise as to the necessity and frequency of this routine.
There are now one-step solutions available that make the hygiene routine even easier. Always remember that if your eyes feel uncomfortable, sore or irritable, you should take your lenses out and make an appointment to see your eyecare practitioner at any of our practices If in any doubt, always seek advice from your practitioner.
I use computers more these days. What is your best advice for my vision?
Vision at the computer
Screen work is strenuous – especially for your eyes. If small visual imperfections are not corrected properly or not at all, then screen activities quickly lead to fatigue, vision problems, tension and headaches. With some people, this added visual stress often triggers migraines unless the eyes are correctly and comfortably focused. Most of the time, these problems can be resolved by spectacles that are correctly adapted for working at the computer. Studies have shown, however, that only about 6% of all spectacles wearers over the age of 45 who regularly work on a screen wear spectacles specifically for that purpose. Correct focus is essential for comfortable vision and we have several ways of giving you that comfort.
The right spectacles
For those affected by presbyopia, reading spectacles are not enough, because they are only suitable for distance in the close-up range up to 36 cm. ”Workplace spectacles” make more sense, which meet the individual requirements of the respective workplace. Special lenses like Ergo® near comfort lenses from Rodenstock are especially well suited. They guarantee smooth vision even in the extended close-up range. For others, who also wear distance lenses, we can help with the right type of multifocal lenses – the most popular being Varilux.
Additional Advice for comfortable work on the screen:
- Look away from the screen now and then, or take small breaks, because short breaks help the eye muscles to relax.
- Adjust the font size on the screen so that everything can be read comfortably without any effort.
- Make sure you blink regularly to avoid dry eyes.
- Pay attention to correct placement of the screen, keyboard and mouse.
- Use the ergonomically correct sitting posture.
- Ensure that there is no reflection from the screen.
- Wear spectacles correctly focused for the viewing distance to the screen.
Can you give me any tips on how to look after my eyes?
The week beginning 21st – 27th September 2020 is National Eye Health Week and has been established to communicate the importance of good eye health under the banner, ‘Vision Matters’. It encourages people from every walk of life to take better care of their eyes and have regular sight tests. This is one of the three priority outcomes of the UK Vision Strategy launched in 2008 by Vision 2020UK. Regular sight tests and OCT eye scans are essential for maintaining healthy eyes but there are other things you can do to look after your eyes.
Diet
Studies show that what we eat can affect our vision. Antioxidants can help to prevent retinal damage. One anti-oxidant which is hugely beneficial is lutein. An OCT eye scan can look for subtle retinal changes that are caused by oxidative stress, much of which can be minimised with proper diet.
Foods recommended for eye health include:
- Broad leaf greens such as kale and spinach
- Brightly coloured fruit and veg such as corn, carrots, orange sweet peppers and oranges
- Oily fish like salmon, tuna and mackerel
- Broccoli
- Eggs
A Feast for Your Eyes (look after your eyes)
Exercise and eyesight
Lack of exercise contributes significantly to several eye conditions, particularly amongst people aged 60 and over. Exercise may reduce the risk of sight loss from narrowing or hardening of the arteries, high blood pressure and diabetes.
Find out more about exercise and eyesight (Royal College of Ophthalmologists PDF)
Alcohol
Excessive alcohol consumption can lead to serious health conditions which can have a detrimental effect on your eye health.
Find out more about alcohol and the eye (Royal College of Ophthalmologists PDF)
Smoking
After ageing, smoking is the biggest risk factor for developing macular degeneration.
Smoking also increases your risk of developing cataract.
Find out more about smoking and your eyes (NHS Choices)
The Sun
Protecting your eyes from the sun is very important and should not be underestimated. Under no circumstances should you ever look at the sun directly. Your sunglasses should have the CE mark on them which ensures that they are giving you the right level of ultraviolet protection.